Effect of a fluid bolus on cardiovascular collapse among critically ill adults undergoing tracheal intubation (PrePARE): a randomised controlled trial. David Janz, Jonathan Casey, Matthew Semler et al. Lancet Journal of Respiratory Medicine. Oct 2019.
Dave Janz is an intensivist at LSU New Orleans who did his Pulm Crit training at Vanderbilt. He started the Pragmatic Care Trials group with Matt Semler and Todd Rice while fellows. This research team recently brought you the PreVENT trial. He’s here to answer a couple questions regarding the most recent trial, PrePARE, and paint the picture of their future trials.
METHODS:
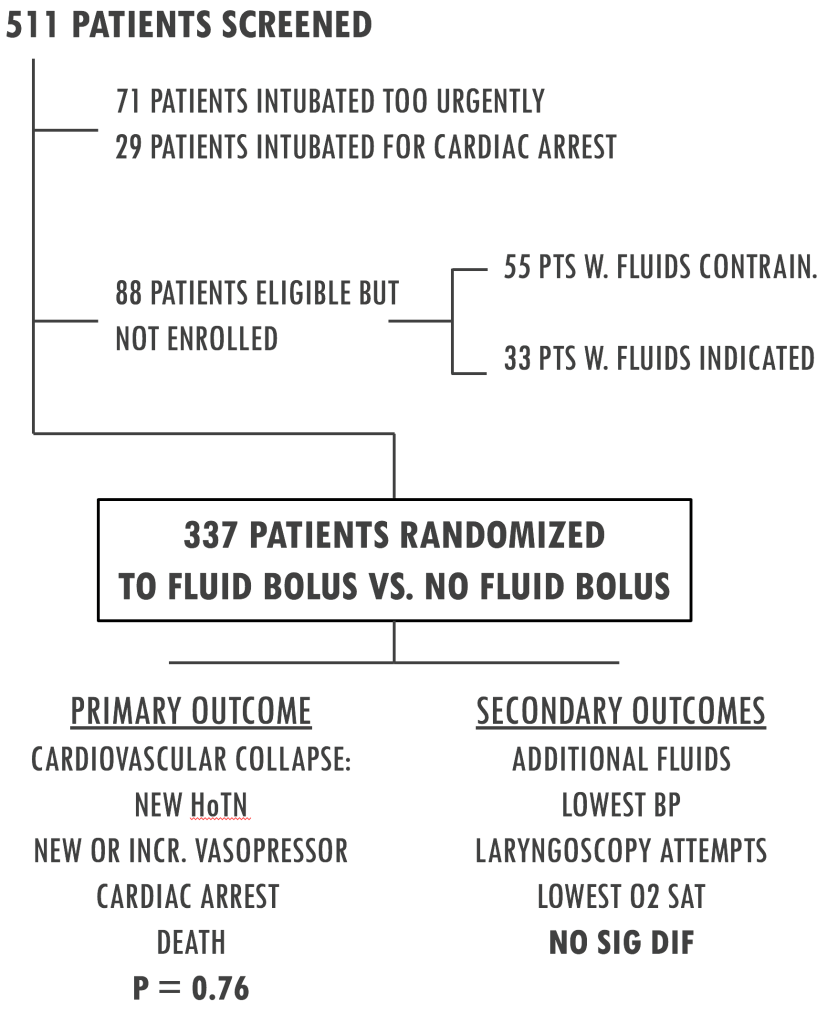
- Prospective, randomized, pragmatic, unblinded study in 8 ICUs and one ED.
- Patients undergoing tracheal intubation were randomized to receive 500cc of crystalloid during intubation. Median fluid received at time of first attempt was 200cc, with the remainder completed after.
- Patients were excluded if the treating physician felt administration of fluids was required or contraindicated.
- Fluids were pressure bagged through induction and laryngoscopy.
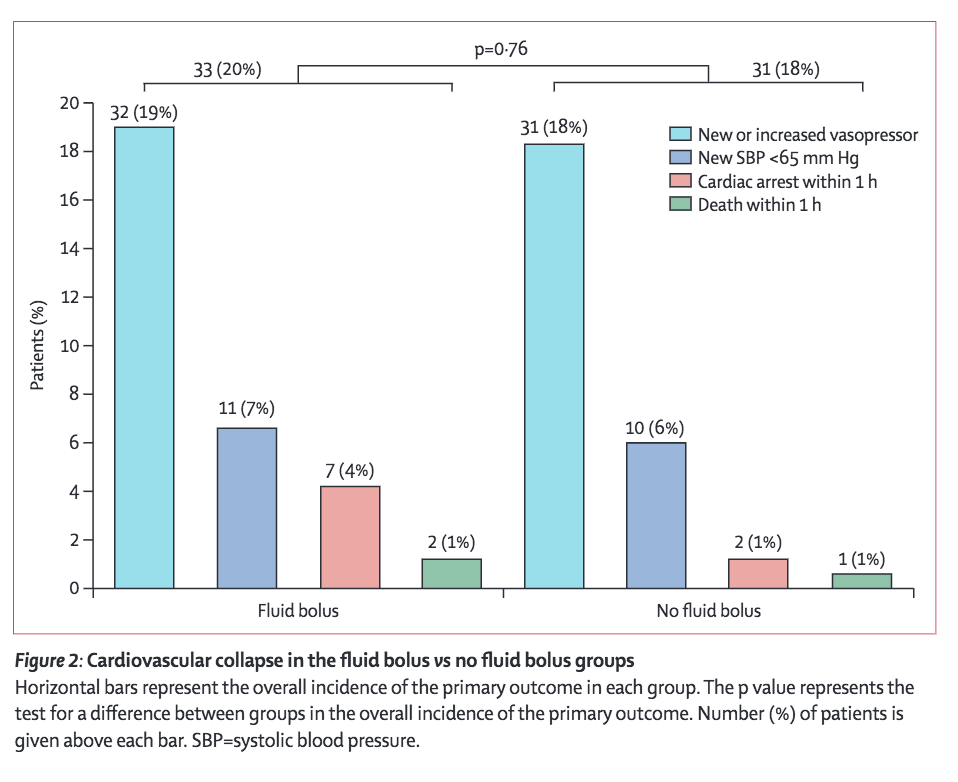
RESULTS:
We see no significant difference in the primary or secondary outcomes with the exception of one subgroup analysis. Patients undergoing PPV at any time during the procedure demonstrated a significant trend towards favoring fluids, while those not receiving PPV actually did worse as seen below. This definitely raises an eyebrow so let’s discuss more with the author.

Interview with Lead Author Dave Janz:
What made you want to study the effects of a fluid bolus during intubation?
Prior to PreVENT and PrePARE, we actually published an intubation checklist randomized trial that was somewhat modeled after the “Jaber” checklist published in Intensive Care Medicine in 2010. That study included a pre-procedure fluid bolus with before and after analyses. We researched the background of what existing evidence there is for using a fluid bolus to prevent cardiovascular collapse. I realized that there were not any randomized trials to try to answer this question. There are lots of observational data out there but no randomized trials. So, that was how we decided to pick fluid bolus as the next thing that we were going to study.
So did it surprise you that a fluid bolus made no significant difference?
Yeah, so anecdotally I’ve always said, “You give a fluid bolus and you see the blood pressure go up.” Why would that not happen? Turns out when doing the background for this study there’s some pretty good animal data and data in adults undergoing general anesthesia that a fluid bolus doesn’t always make the blood pressure go up and sometimes actually makes the blood pressure go down. But clearly our hypothesis was that this was going to increase the procedural blood pressure compared to no fluid bolus. Furthermore, in the PrePARE trial the rate of cardiovascular collapse was actually numerically higher in the fluid bolus group, so we had to think why that would be.
The other thing you reported was that only 200cc of the bolus was given prior to induction. Would you have liked to see more, maybe to increase the signal?
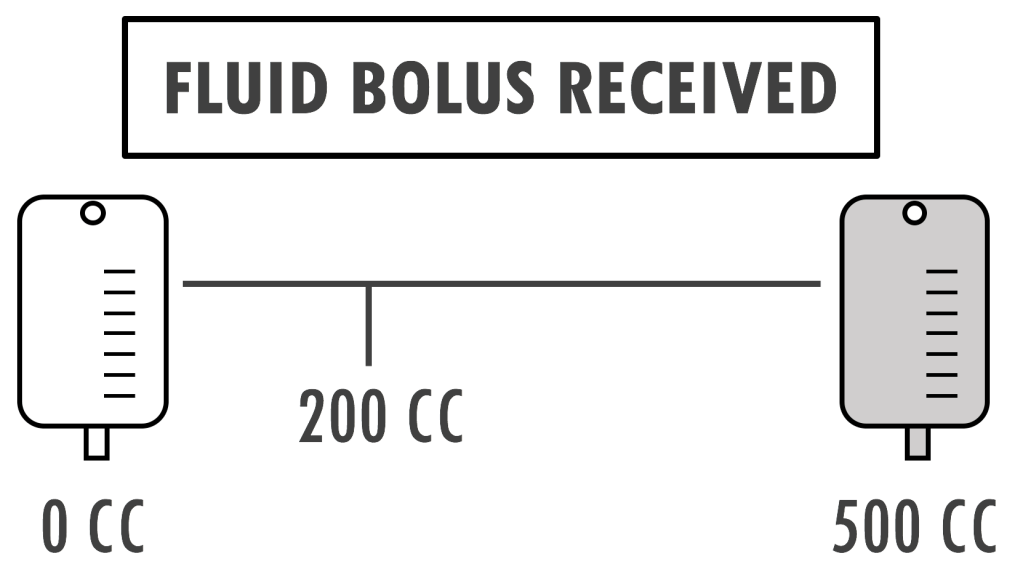
The way the trial was set up is that the only thing that protocol was guiding is that you had to start the fluid bolus prior to induction drugs being given. The protocol did not say how much fluid had to be infused by the time the drugs were given. The most common amount of fluid in the prior observational studies was 500cc and the most common way the fluid was given was just starting the fluids prior to induction. So this actually reflects common practice and if there’s a problem with that, then it’s not just with our study but with general practice. It’s true that this is a potential reason there’s a null effect, but the fact is that our trial behaved the way everyone else behaves with these fluids.
One of the most interesting parts of your study is that the patients who were getting positive pressure ventilation showed a decrease in collapse, which we would expect. However, patients who were not receiving positive pressure ventilation actually had an increase in cardiovascular collapse. How do you reconcile these findings?
That’s a good question. I was hoping you would answer that question for me. This was another result that was completely unexpected. We chose these subgroups intentionally because we thought fluids were likely to have the biggest effect on patients with positive pressure ventilation and this is supported by the subgroup analysis. But what we did not expect; how in the world would a fluid bolus provoke cardiovascular collapse in a patient not receiving PPV. Of course these are hypothesis generating findings and don’t prove anything. They only suggest where the signal may be.
Regarding your practice and with consideration of your trial, the PreVENT study, are you routinely bagging during the apneic period, in the absence of any contraindications?
I personally think it should be the standard of care when you’re intubating patients in the ICU. As long as they’re not actively vomiting or what not, everyone should be bagged. The question is should everyone be getting a fluid bolus. I don’t think we have enough information to answer that entirely. However, I think I would be at least a little worried about giving the fluid bolus to someone you don’t have on positive pressure ventilation. While these are hypothesis generating signals, it will at least make you reconsider making a fluid bolus as part of standard of care in patients not being bagged.
These signals actually prompted PrePARE 2 which started enrolling approximately a year ago. Patients are being randomized to a fluid bolus or none only if they are getting bagged and/or non-invasive positive pressure ventilation. None of the investigators are interested in studying fluid bolus again in patients not being bagged, since that makes us worry too much…
I suppose it’s not necessarily the most ethical trial to prove that we’re causing cardiovascular collapse with fluids...
But hopefully we’ll have an answer to what standard of practice should be when it comes to fluid bolus in patients receiving positive pressure ventilation.
Anything else on the horizon?
The other trial we have ongoing is about a quarter of the way through, it’s called BOUGIE. It’s going to be a multicenter trial validating the BEAM trial by Brian Driver. Clearly the BEAM trial proved that in the ED, at Hennepin County, where you have people trained in the bougie, bougie use is better than not. But what we want to know is does the bougie work everywhere, meaning does it improve outcomes in operators who have only used it 5 times. This trial is going to enroll about 1000 patients in ED and ICUs.
Authored by Terren Trott @tsquaredmd, peer-reviewed by Chris Belcher @seebelcher236
RELATED:
PulmCrit Wee: Do fluid boluses before intubation help? (PREPARE trial). Josh Farkas, PulmCrit
PrePARE: Effect of Fluid Bolus on CV Collapse During RSI. Anand Swaminathan, Salim Rezaie. RebelEM.
REFERENCES:
- Janz et al. Effect of a fluid bolus on cardiovascular collapse among critically ill adults undergoing tracheal intubation (PrePARE): a randomised controlled trial. Lancet Respir Med. 2019 Oct 1. pii: S2213-2600(19)30246-2
- Jaber et al. An intervention to decrease complications related to endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Intensive Care Med. 2010 Feb;36(2):248-55
- https://5minuteairway.com/2018/06/11/beam-article-with-brian-driver-interview/
- https://5minuteairway.com/2019/03/06/prevent-trial-and-interview-with-jon-casey/
