
The hyoepiglottic ligament is arguably the most important ligament in the human body with its sole purpose being to help you intubate the most challenging of airways. Perhaps a slight exaggeration, but nonetheless, management and manipulation of the hyoepiglottic ligament is important in airway management.
What is it?
The ligament connects the hyoid bone to the epiglottis and functions primarily during swallowing to allow the epiglottis to close over the glottis. In airway management, it’s your target within the vallecula for Mac blade engagement.

How To Use it.
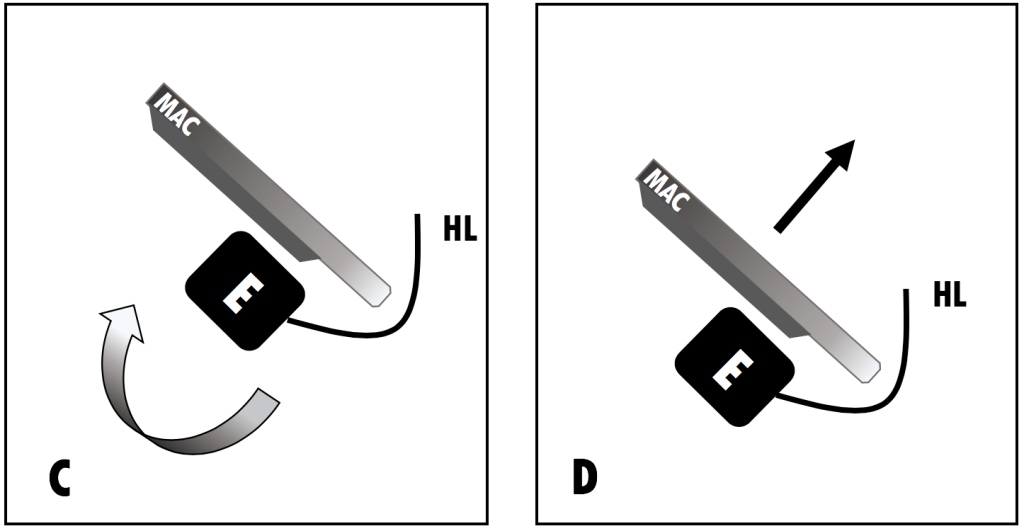
Tension on the ligament results in retroversion of the epiglottis and visualization of the cords underneath. Pivoting the epiglottis typically requires minimal force and only small movements. Once the epiglottis is out of the way, lift to displace the base of the tongue and soft tissue. Below is a sagittal graphical representation.
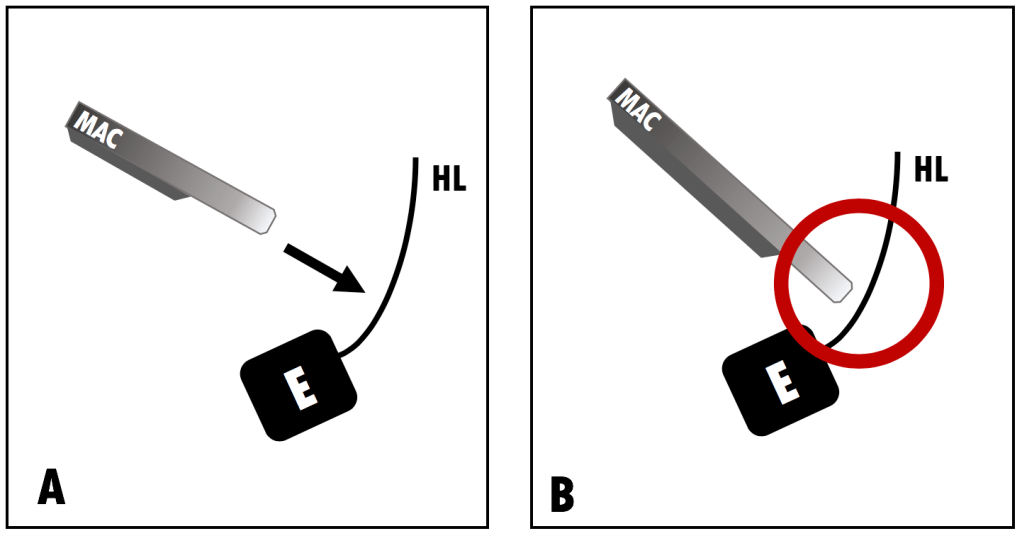
A. Your Mac blade entering the vallecula and targeting the hyoepiglottic ligament. B. Engaging the hyoepiglottic ligament.
C. Retroversion of the epiglottis with pressure on the hyoepiglottic ligament. D. Only once activated, lift the soft tissue out of view.
In real life, we see the retroversion of epiglottis caused by the Mac blade engaging the ligament and then dunked on hard.
Next, staying engaged when the tube is passing will help avoid the classic “grade III drop” just as the tube is tugging on the glottis, as in this example below, seen at 0:28.
In this clip we see the hyoepiglottic ligament engage well and then lose traction once the tube starts to pass. You can see clearly towards the end of the clip, the hyoepiglottic ligament and the Mac blade superior to it. This results in us losing the view right as the tube passes.
How To Do It Wrong.
Inappropriate engagement or lateralization results in a skewed angle of the larynx. This can be especially pronounced with an angled approach of the laryngoscope. Whether you use a “down the middle” or “sweep the tongue” technique, you’ll want to be conscientious of the angle of engagement with the hyoepiglottic ligament.
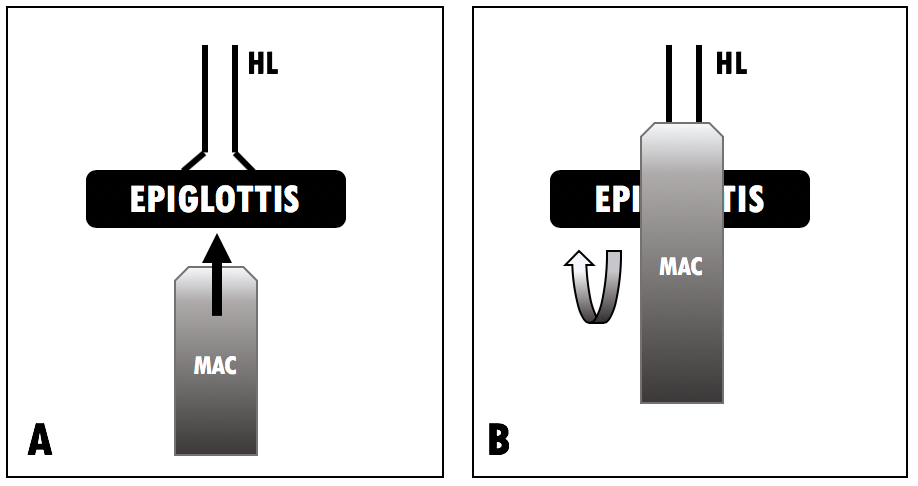
Here we see the hyoepiglottic ligament just missed by the tip of the Mac blade. This results in the larynx skewed off axis and an oblique view of the cords.
This example demonstrates the same concept but to a less degree. Not quite perfect engagement but we’re still able to get the job done nonetheless.
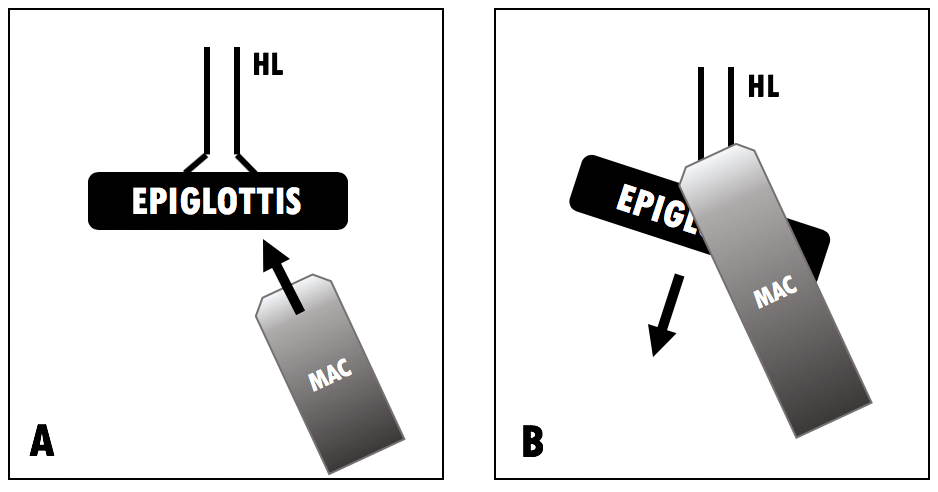
Next we see that lifting too early or not engaging the hyoepiglottic ligament will not expose the glottis, like in this example of a coding patient.
In this case, we have no view of the cords and we can clearly see the hyoepiglottic ligament unengaged. Either reach a little deeper with the blade tip or if using a Mac 3, perhaps it’s time to reach for the Mac 4.
Summary and Pearls:
- Use the hyoepiglottic ligament to your advantage; activate with the tip of the Mac blade to reveal the glottis.
- Keep the ligament engaged when passing to the tube to keep a good view.
- An off-axis approach can skew the larynx and worsen your view.
- Not engaging or lifting too soon will often result in a worse view.
Written by Terren Trott (@tsquaredmd) and reviewed by Chris Belcher (@seebelcher236)
