
Bag-Mask Ventilation during Tracheal Intubation of Critically Ill Adults. New England Journal of Medicine. Jan 2019.
Jon Casey is currently a fourth year fellow in CCM at Vanderbilt. He did a chief year followed by a hospitalist year at Brigham and Young prior to making the move to Vanderbilt. The group at Vanderbilt is working to challenge concepts in routine care and see if the data can back up our practices. The projects range from fluids, to contact precautions to airway management. The current study challenges the dogma that bagging during the apneic period is dangerous. Jon Casey discusses how the study has changed his management of critically ill patients and challenges some of the criticism of the study below.
Methods:
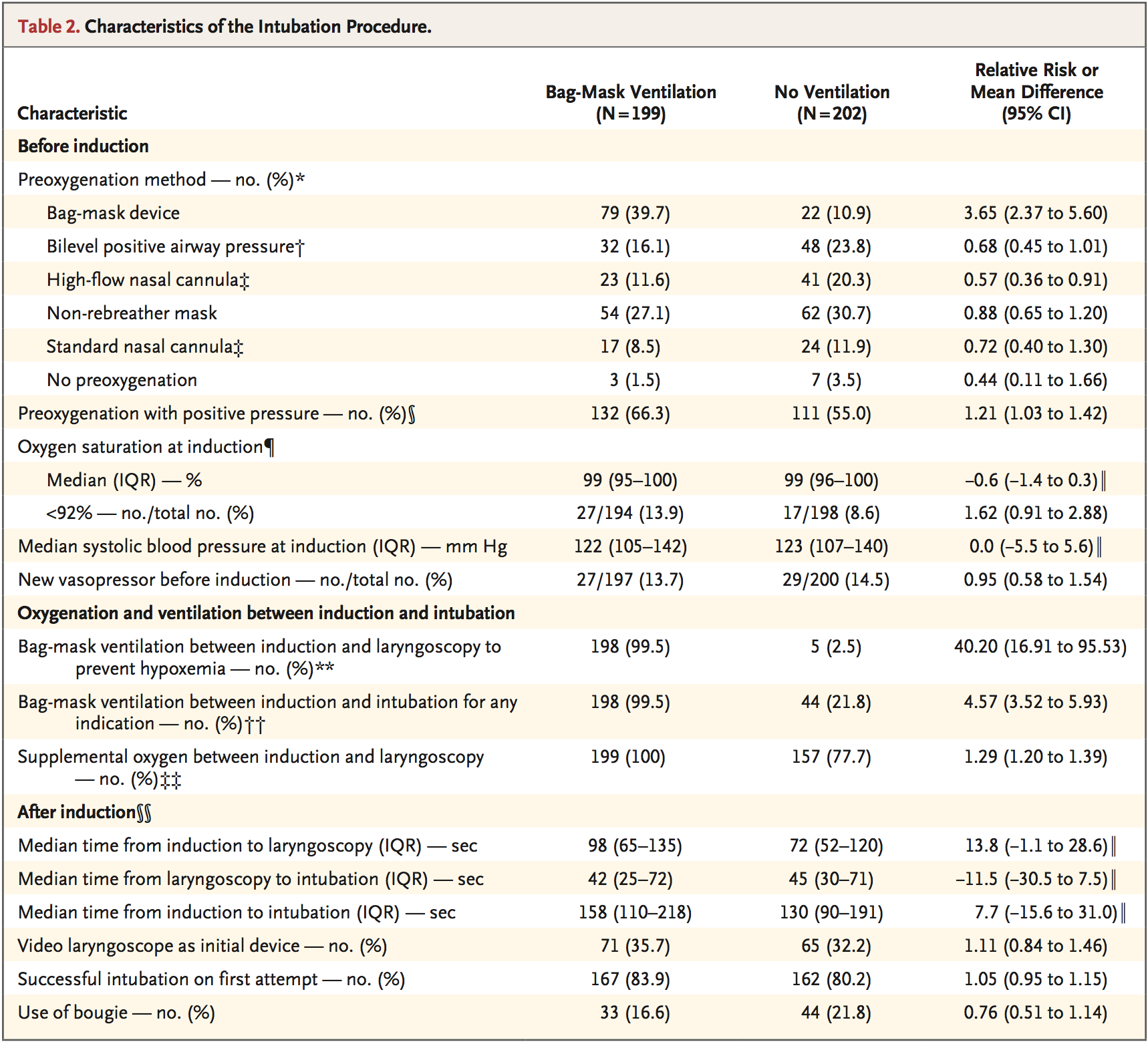
401 ICU patients were randomized to receive either BVM during the apneic period or no ventilation at all. Meaning after induction was pushed, patients were bagged until the first attempt at laryngoscopy. In the no ventilation group, BVM could be used after failed attempt, desaturation or for patient safety.
PreVent Trial Recommended BVM Technique
Two-hand BVM with 15 LPM or greater
PEEP valve with 5-10 cmH2O PEEP
Oropharyngeal airway
Head tilt and chin lift maneuver
RR of 10
Smallest volume to see visible chest rise
Of 667 patients screened, 401 met enrollment criteria. Exclusion criteria included patients who required rescue BVM for hypoxia pre-intubation, other indications for BVM such as severe acidosis or, reversely, indications not to bag, such as ongoing vomiting and hemoptysis.
Other interventions, such as apneic oxygenation and pre-oxygenation technique were left to the discretion of the physician. In patients in the no-ventilation group failed first pass attempt, they weren’t allowed to be bagged until SpO2 was <90%.
Outcomes and Results:
Primary outcome: median lowest saturation during intubation and up to 2 minutes afterwards
With BVM: 96% (IQR: 87-99) versus No Ventilation: 93% (IQR: 81-99%)
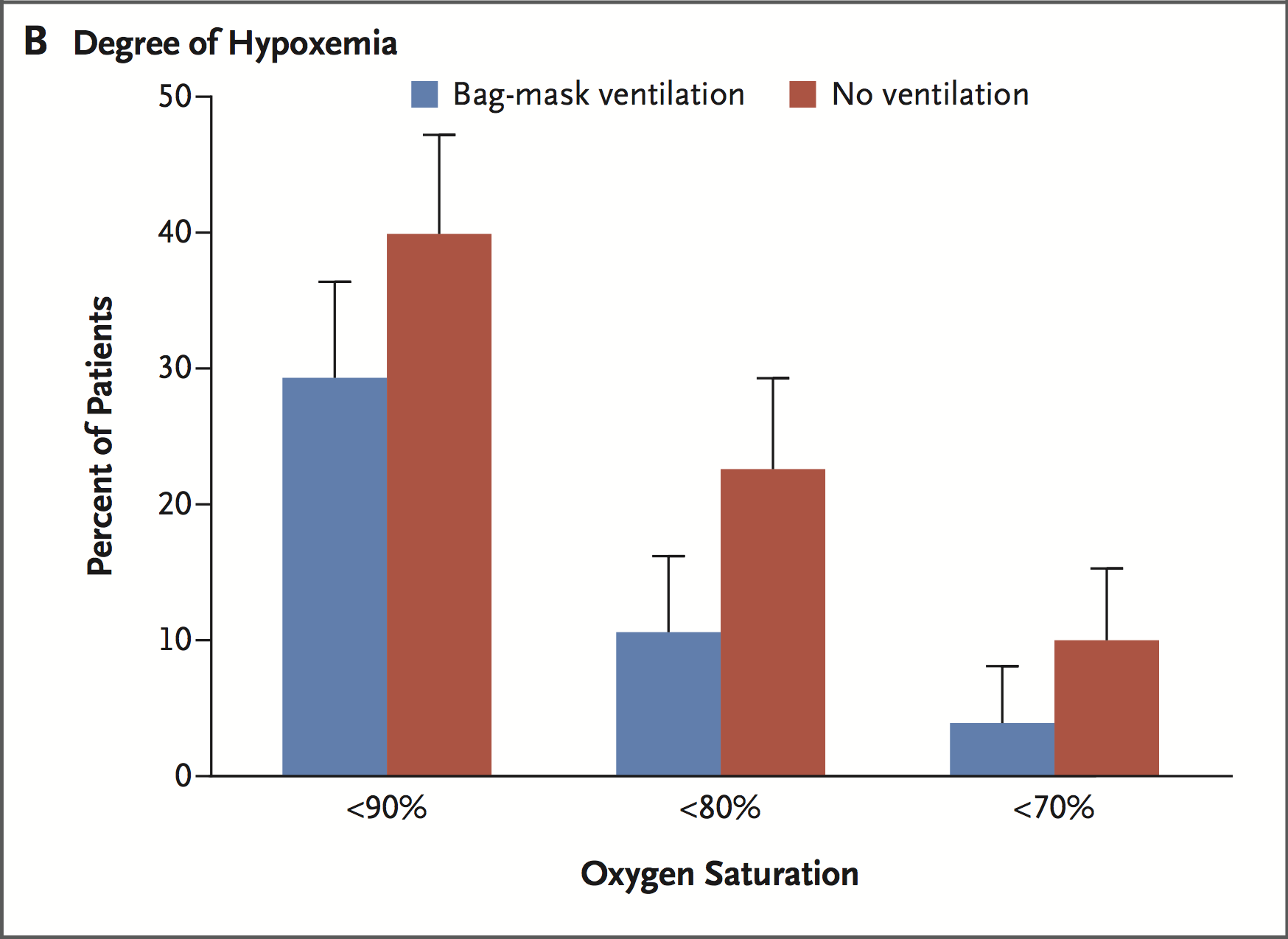
Secondary outcome: incidence of severe hypoxia, measured less than 80%
With BVM: 10.9% versus No Ventilation: 22.8%
Operator Reported Aspiration:
With BVM: 2.5% versus No Ventilation: 4%
Discussion:
First, this is a well done study that actually reflects our patient population. This study addresses two key points: prevention of critical desaturations during intubation and indirectly, addresses risk of aspiration. As described, the BVM technique is critical: using minimal TV to detect chest rise at a respiratory rate of 10 breaths per minute. This means these patients weren’t being over-aggressively bagged and hyperinflated. Not only does this demonstrate that a preventative, ‘calmer,’ technique is able to prevent critical desaturations, it’s a stark contrast to the rescue ventilation technique that inevitably leads to gastric insufflation and a couple beads of sweat.
The median lowest saturation between the groups isn’t that different but largely this is because the majority of patients have uneventful intubations; I wouldn’t have expected a very large difference. Key is the incidence of critical desaturations between the groups, in which BVM during the apneic period confers a clear benefit. Furthermore in the subgroup analysis, there was even more benefit to patients requiring higher FiO2 prior to intubation or couldn’t be preoxygenated >97%.
While this study wasn’t set out to stomp the debate that BVM causes aspiration it does provide some insight. In patients who don’t have obvious contraindications to BVM, it appears to a safe technique. I think judicious patient selection is key and I’m a huge fan of monitoring your peak flow while bagging, provided your BVM has that device.
Interview with Jon Casey:
What exactly made you want to do this study? I mean it’s a pretty significant undertaking; it was seven ICUs across multiple institutions. So why was this particular question important?
We felt like tracheal intubation was something that we do a lot in the ICU, but we don’t have much consensus on the right way to do it. It’s a two-minute procedure with a 2-4% rate of cardiac arrest, yet most people do it basically the way it was first described 50 years ago. Within this short procedure, there are numerous controversies: choice of induction medication, cricoid pressure, ventilation, patient positioning, and equipment. And there is not much data to help providers choose between all of the various options.
Over the last five years our group has attempted to study some of these controversies and in the process, we have built a network of other investigators in critical care, emergency medicine, and anesthesia who are willing to volunteer their labor to figure out the best way to perform emergent airway management. Many of our ideas have come from the huge variability in standard practices between centers and provider specialties.

Aaron Joffe, one of our collaborators at the University of Washington, provided the original idea for the PreVent trial. At the SCCM conference three years ago, he described his approach to intubation and said “well you know I do X, Y and Z and of course I bag-mask ventilate every patient.”
And to us that was mind blowing. We had tended to follow strict RSI and did not routinely provide bag-mask ventilation. Data from our previous trials, however, showed that Aaron was far from alone as ventilation was used in about 50% of intubations at our sites.
To some of our collaborators it sounded like common sense, and to others it sounded heretical. So, we tried to find the data for this foundational piece of strict RSI technique, and we discovered that no trial had ever evaluated the safety or efficacy of bag-mask ventilation during emergency airway management.
When I was doing research for this I really couldn’t find very much clinical reference in terms of who can be bagged and who can’t be bagged. There’s really not that much out there.
It’s all really expert opinion. The only data that existed were studies of healthy patients, in the operating room, in whom providers bagged with varying pressures and asked, “How hard do I have to bag to hear air the stomach?” It seems amazing that one of the biggest decisions during one of most common procedures we do in critically ill patients is based on studies of medical student volunteers from the 1950s. To our knowledge, the PreVent trial is the first trial of prophylactic bag-mask ventilation during emergency airway management.
So was there a pretty significant change in the culture of BVM at Vanderbilt before the trial was done and now after? Or was it kind of something you’re already doing but you wanted to back it up.
The majority of providers in the PreVent trial are pulmonary critical care trained and, although there was a spectrum of practice, the minority of providers was routinely providing bag-mask ventilation every time. So the results of the trial do represent a significant change for many of the providers who were not routinely providing bag-mask ventilation every time, and are now incorporating that into their practice.
So who falls into your patient selection for who can be bagged and who can’t, with the results of this study?
Our trial was conducted in intensive care units. We stated that patients should be excluded if bag-mask ventilation was required or unsafe to provide. We allowed providers to choose what criteria made patients so high risk for aspiration that ventilation was unsafe. In the end, only about 7% of patients were excluded for high risk of aspiration. That may not be the same in every setting, and many people question if these results apply to patients intubated in the ED or pre-hospital setting. However, patients in the PreVent trial were at significant risk of aspiration, with 60% having at least one risk factor, and only 50% of patients being known to be NPO. In the ICU, I think most patients should be eligible to receive bag-mask ventilation.
Some of the criticism of the study is that you’ve demonstrated something that we already, intuitively, knew; bagging prevents desaturations, what would be your response to that?
Although it is not entirely surprising that bag-mask ventilation helps oxygenation, prior to the trial we heard many people suggest the period between induction and laryngoscopy was too small to have any meaningful effect. And we have also seen other “intuitive” interventions during tracheal intubation, like apneic oxygenation, struggle to affect oxygenation in the way we assumed they would. However, I think the big surprise of our trial for many people, and what I found surprising as someone who did not routinely provide bag-mask ventilation before the trial, was how effective bag-mask ventilation was at preventing severe cases of hypoxia. For anyone who says this was obvious and we knew this already this, that doesn’t seem to be reflected in guidelines of emergency airway management or surveys of what current practice looks like. If you look at UptoDate today, it recommends not providing prophylactic ventilation. Jesse Ehrenfeld published a survey of US anesthesiologists (link below) which showed less than half of anesthesiologist reported providing ventilation after administration of neuromuscular blockade, and our impression is that few emergency medicine doctors routinely provide bag-mask ventilation.
If it was obvious that bag-mask ventilation was effective and safe, then why weren’t people doing it?
So while your study wasn’t designed to prove that BVM is safe regarding risk of aspiration, how can we extrapolate some of your findings to that debate?
This is one of the largest trials of emergency airway management ever completed. If you wanted to definitively know the effect of bag-mask ventilation on aspiration you’d have to have a trial of 4000 people. And we don’t we don’t have a trial like that right now. While the PreVent trial doesn’t definitively determine the effect of bag-mask ventilation on aspiration, it provides some guidance. The 95% confidence interval for the effect of bag-mask ventilation on the risk of aspiration seems to be somewhere from a 4% decrease to a 2% increase. So you’re talking about either no effect on a rare outcome or a small effect on a rare outcome, compared to a big benefit in preventing hypoxemia which is common and appears to be a major driver of peri-procedural cardiac arrest.
In practice, do you employ any strategies clinically to reduce your risk of aspiration?
I think prophylactic bagging may be different than rescue bagging. So if you have a difficult airway that takes 14 minutes with three attempts from multiple different operators, I think it’s not it’s not hard to imagine that vigorous bagging for a prolonged period of time could cause aspiration. The CAAM study, recently published in JAMA, comparing bag-mask ventilation to tracheal intubation during out-of-hospital cardiac arrest suggested that bag-mask ventilation may increase the risk of aspiration, but that was a different intervention. In the CAAM trial, rescue ventilation with a bag-mask device was provided for 15 to 30 minutes. In PreVent, we did not see the same effect, but patients received only 1 minute of gentle, prophylactic bag-mask ventilation.
I think it certainly seems possible based on our data that one minute of gentle, prophylactic bag-mask ventilation may not increase the risk of aspiration, at least not in the vast majority of people. Personally, I pay careful attention to airway patency maneuvers during bag-mask ventilation and also ensure that only enough volume is provided to generate a chest rise. The role for cricoid pressure and ramped position in preventing aspiration is probably a debate for another day.
Then on to pre-oxygenation. There’s been quite a few studies out recently regarding the best technique. What’s your approach?
I will say that, in general, that the collective weight of the evidence is that ventilation with positive pressure prevents hypoxemia. Positive pressure can be provided with BiPAP or with a bag-mask ventilation with a PEEP valve. The great thing about bag-mask ventilation is, it’s always there. BiPAP, especially the emergency room, is not always available. Even in the ICU you may not have time to bring a vent into the room. With a high risk patient, using BiPAP for preoxygenation and for ventilation from induction to laryngoscopy may be the best approach.
BiPAP has several advantages, including ensuring that breaths are provided at controlled and not excessive pressures.
Last question. Do you feel like this study makes a lot the apneic oxygenation via nasal cannula, kind of a moot point? In some ways, this study silences that route of research.
I think the jury’s out on whether apneic oxygenation helps to prevent hypoxemia at all. The weight of evidence has been mixed but certainly there’s been no trial of apneic oxygenation during emergency airway management that shows it’s dramatically effective. This trial of ventilation seems to be so effective that I think it answers the debate: in patients for whom it’s safe to bag, you should bag. In the 10 percent of ICU patients who you don’t think it’s safe to bag, I think applying supplemental oxygen during laryngoscopy is reasonable.
Our first trial, the FELLOW trial, didn’t show a benefit of apneic oxygenation. The ENDAO trial out of the Lincoln Medical Center Emergency Department similarly didn’t show any benefit of apneic oxygenation. Trials of high flow nasal cannula, like the PREOXYFLOW trial also haven’t shown a large difference, but it may still provide some benefit. In general, I think any benefit of apneic oxygenation with nasal cannula, high flow or not, is so dramatically outweighed by benefit of bag-mask ventilation, there shouldn’t be a debate for a patient who’s eligible for bag-mask ventilation.
Once free of fellowship, what’s in your future?
So I’m joining the faculty at Vanderbilt on July 1st and we’re doing more of these comparative effectiveness trials. We have a couple trials on intubation; we have one using a fluid bolus to prevent peri-procedural cardiovascular collapse. We’re doing a multicenter trial with the group from Hennepin, validating the BEAM trial. So, in terms of airway management those are the next two things we’re doing. We have real interest in looking at choice of induction drug at some point. Ketamine versus etomidate. We’re also looking at other things that are important for critical ill patients and are similarly areas of controversy. On April 1st, we conclude the PROPER trial, a trial of protocolized post-extubation respiratory support. We’re trying to develop methodologies to answer these highly debated questions about interventions that are already routinely used in usual care.
Congrats again on your publication and looking forward to seeing these studies in print when they’re done.
Terren Trott @tsquaredmd
References and Links:
![]() Jonathan D Casey et al. Bag-Mask Ventilation During Intubation of Critically Ill Adults. NEJM 2019.
Jonathan D Casey et al. Bag-Mask Ventilation During Intubation of Critically Ill Adults. NEJM 2019.
![]() Ehrenfeld J. et al. Modified Rapid Sequence Induction and Intubation: a survey of United States Current Practice. Anaes and Analgesia 2012.
Ehrenfeld J. et al. Modified Rapid Sequence Induction and Intubation: a survey of United States Current Practice. Anaes and Analgesia 2012.
![]() Semler MW et al. Randomized Trial of Apneic Oxygenation During Endotracheal Intubation of the Critically Ill. Am J Respir Crit Care Med 2015
Semler MW et al. Randomized Trial of Apneic Oxygenation During Endotracheal Intubation of the Critically Ill. Am J Respir Crit Care Med 2015
