EmergeNcy Department use of Apenic Oxygenation versus usual care during rapid sequence intubation: a randomized controlled trial.
Caputo et al. Annals of EM, Aug 2017
Nick Caputo works at Lincoln Medical Center, a single ED with 175,000 visits a year. He did a general surgery internship, an emergency medicine residency at Lincoln Medical Center and a Critical Care Retrieval fellowship in Australia. He’s now published the second prospective study showing no difference in O2 sats with apneic oxygenation. Check out the Q&A below.
Introduction:
Pre-oxygenation is a pretty rock solid concept. Flushing out as much ambient air and replacing with oxygen has been shown to prolong time to desaturation during intubation. Apneic oxygenation is another concept with a little more tumult. Studies conflict as to whether or not supplemental oxygen during the apneic period of RSI prevents desaturations or other patient-centered outcomes. This study aims to answer this definitively, as it’s an emergency department population, prospectively collected and randomized – but is this the study to nail the coffin of apneic oxygenation?
Outcomes measured:
The primary outcome was the average lowest oxygen recorded during intubation with secondary outcomes including differences in first pass success, desaturation to 90% or 80% and time to desaturation.
Methods:
This was a prospective study performed at single academic center in New York. Two hundred patients were randomized to either apneic oxygenation by nasal cannula at >15LPM or no supplemental oxygen during laryngoscopy.
|
200 patients enrolled |
|
All patients receive minimum 3 minutes of pre-oxygenation via 15L/min NRB, BVM or BiPAP |
|
100 Patients with Apneic Oxygenation by NC >15LPM |
All patients received a minimum of 3 minutes of pre-oxygenation with NRB, BiPAP or BVM, if patients were not pre-oxygenated they were excluded (18 patients). A third party recorded data points including lowest oxygen saturation. The apneic period was defined as the time the blade was inserted into the mouth to the time any other form of oxygen was supplemented. All other aspects of intubation were not controlled.
Results:
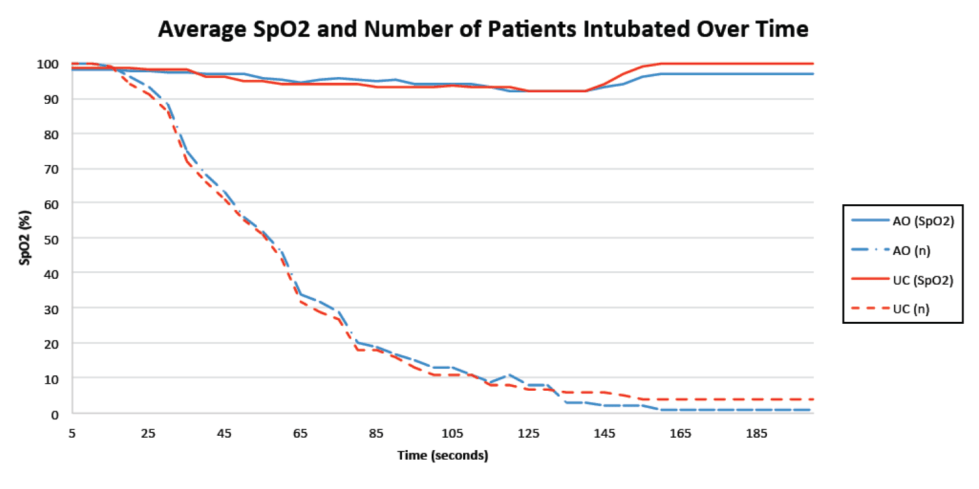
Caputo et al. observed no difference in lowest mean arterial saturation between the ap-ox and usual care groups. Furthermore, all patients were intubated by 195 seconds and there was no difference at saturations at any time point. Also notable, patients who had multiple attempts, ie a more difficult and longer intubation, or multiple attempts without ‘re-ventilation’ had no difference in lowest SpO2.
Mean Lowest SpO2
With apneic oxygenation 92%
Usual care 92%
P= 0.08
Other outcomes, including number of patients below 90%, below 80%, mortality rates also did not differ.
Discussion:
This is the first study to look at the use of apneic oxygenation in an ED population. Very similar to the FELLOW trial, we’re seeing no difference in lowest mean SpO2 with apneic oxygenation during intubation. This study is unique in that all patients were pre-oxygenated, and for an average of 13 minutes, prior to intubation and 15 patients were excluded for lack of pre-oxygenation. Intubations were performed fairly quickly with the majority being done in 60 seconds and all done by 195 seconds. What seems to be very evident, is that for most intubations, with pre-oxygenation the role of apneic oxygenation is pretty limited.
This study brings to light two populations that the role of apneic oxygenation may still be useful, those not able to pre-oxygenate and those with exceptionally prolonged apneic periods. Despite the indication for intubation being primarily pulmonary (~60%), all were stable enough to receive pre-oxygenation and on average quite a bit of pre-oxygenation. This makes me think that even these patients with pulmonary indications hadn’t already dropped off their dissociation curve, which happens to be the population that gets us most on edge. Could apneic oxygenation benefit these patients? Secondly, what about the rare patient that exceeds a 3-minute apneic period? That’s clearly a challenging intubation and perhaps apneic oxygenation would provide a longer time without desaturation. However, to argue against myself, perhaps if you’re getting into a 3-minute apneic period during an intubation, its time to bag them and change your approach. Let’s hear from Nick Caputo on his thoughts..
Interview with Nick Caputo, MD, lead researcher:
Is airway research a topic you’re particularly interested in?
When I got into administration, one of the things I learned about was root cause analysis and quality improvement. We found out pretty early on, that we didn’t have a really good grasp on airway and we had a lot of cases under scrutiny. One of the things we did is we went around and asked the residents and attendings what RSI was. They all said basically the same things: pre-oxygenation/preparation, induction/laryngoscopy and intubation (passing the tube). We then directly observed 100 intubations and we found that our own faculty and residents weren’t adhering to what they said the process is, with the biggest fallout being pre-oxygenation. Only about 50-55% of the time were they doing correct pre-oxygenation. So were like shoot, this isn’t good, especially with being in the ED constantly being under the microscope.
So we looked at where we were excelled and where we were falling behind and we developed a 31 point checklist. We really designed the checklist to bring the temperature down in the room. This is because one of the things we observed was that people were creating emergency out of urgency. People were like, we have to get the airway now, now, now when it was like, calm down everyone, there’s time to prep and do everything. Furthermore, the checklist takes at least 3 minutes to complete the steps to induction; this ensured that there was at least 3 minutes of pre-oxygenation. While we were rolling this  out a bunch of the residents were talking about apneic oxygenation and where this falls into play. A couple of the attendings met and we went through the literature on it. It seemed as though people were really pro ap-ox without actually having a good scientific basis for it in the ED. It sounds good in theory and it works in the operating room, but what about our patients? We looked at the FELLOW trial that Matt Semler did in the ICU, and one of the criticisms of that trial was that you had people saying, that’s great for the ICU but those aren’t ED patients. The residents follow social media much more than a lot of attendings do, so they were really gung-ho about it. As a department, we really had to be critical of it, because we strive to apply evidence based medicine and best practices to the bedside. One of the ways we do this is we test these best practices in our own population. In this way, we figure out whether or not these practices work for our patients, we learn about our patients and the residents learn about how to design research and tests hypotheses. So we designed the ENDAO trial, but before we kicked it off we had a long conversation with Matt Semler from the FELLOW trial and asked him what his obstacles and criticisms were in order to try and improve on his study.
out a bunch of the residents were talking about apneic oxygenation and where this falls into play. A couple of the attendings met and we went through the literature on it. It seemed as though people were really pro ap-ox without actually having a good scientific basis for it in the ED. It sounds good in theory and it works in the operating room, but what about our patients? We looked at the FELLOW trial that Matt Semler did in the ICU, and one of the criticisms of that trial was that you had people saying, that’s great for the ICU but those aren’t ED patients. The residents follow social media much more than a lot of attendings do, so they were really gung-ho about it. As a department, we really had to be critical of it, because we strive to apply evidence based medicine and best practices to the bedside. One of the ways we do this is we test these best practices in our own population. In this way, we figure out whether or not these practices work for our patients, we learn about our patients and the residents learn about how to design research and tests hypotheses. So we designed the ENDAO trial, but before we kicked it off we had a long conversation with Matt Semler from the FELLOW trial and asked him what his obstacles and criticisms were in order to try and improve on his study.
Why do you think your study has such different results from the OR studies?
The studies out of the operating room are very small in enrollment numbers. One of the residents sent me the Rory Spiegel criticism saying we didn’t find the difference that the OR studies did was because we under powered our study, not for lowest mean arterial saturation, but for rates of desaturation. And I disagree with that because those studies were very small in number and they weren’t powered at all. They fall victim to the theory of small numbers. If I have 40 patients enrolled in a study, then each patient accounts for more than 2% of a change. If I have one patient that desaturates then that’s 2.5% percent rate. It makes it sound like a bigger difference than it truly is. So, number one, those are really small studies and number two, they were fairly healthy individuals. These were elective intubations, they weren’t patients being intubated for primary pulmonary pathologies and to me it made sense. If I have a healthy individual undergoing a procedure and I do proper pre-oxygenation with that healthy patient and have end tidal O2 to confirm that I have done proper pre-oxygenation, then I am confident that I have washed out all the nitrogen. This alone should make for prolonged apnea times regardless of Ap-ox.
How would you respond the fact that in your study, patients were intubated fairly quick so perhaps there wasn’t time to show the difference?
I actually agree with that, but that’s the whole purpose of our study- the purpose being to determine whether or not ap-ox works in a real-world setting. It’s neither here nor there if you give a treatment to everyone knowing that it only works in a specific situation. Ap-ox is supposed to work in patients with really long apneic times. This is generally equated to difficult airways. I’m not so sure I agree. I have been faced with very difficult airways (both anatomically and physiologically) that I have intubated in less than a minute and I have seen really easy airways that have taken longer than a minute by novice intubators. I think that we can’t predict how long or how quick an intubation will be. I really think it should be about how well we are able to pre-ox. If you can pre-ox well, probably no need for Ap-ox, if you can’t, then you probably need it. The initial timing in my opinion comes down to how we pre-ox. Our intubation times are 60, 90 and up to 195 seconds. People will say that’s really quick but when I think about it, that’s a really long time. Sit in your chair and count to 60 and mentally go through the steps of intubating from insertion of the laryngoscope to visualizing the cords to passing the tube. By the time this is done in your mind you’re probably at 30 seconds counting out loud. So to have several minutes of apnea time during an intubation, even if it’s a difficult intubation, is puzzling to me. If I put the blade in and have a grade 4 view on DL then I’m not going to make an attempt. I’m going to switch out to VL and if I still have a difficult view, then I’m going to abort, perhaps place an LMA and think about what my next approach is. I’m not going to risk a prolonged apnea time as well as the subsequent edema that occurs from manipulating the glotic tissues. One has to question if a look is taking longer than 3, 4, 5 or even 6 minutes.
Yeah that’s an intubation not going so well.
We emphasize first pass success and, again, every time you take a look or manipulate the airway you cause edema. Those tissues swell really quickly. Each time you make an attempt you’re making it harder and harder. One of the things we do, is we don’t allow our residents or faculty to attempt unless they have good view. So, if it’s a grade 1 view, go ahead and get in there. If it’s a grade 1 view it shouldn’t take you longer than 30 seconds. If it’s a grade 2 or 3 view one of the things we stress is using a bougie. If it’s a grade 4 view, we tell our residents and attendings, don’t even attempt, switch to video if you haven’t already done so, bag the patient up and think of a new approach. The last thing you want to do is the same thing over and over; you have to change something. I don’t understand the programs where you’re allowing a novice multiple attempts in sick patients that may be making for 6 minute looks. I’m not comfortable with that. Would you want someone, like a novice, taking a 5 to 6-minute look if you’re super sick?
Has this changed your management? Were you guys using apneic oxygenation before and now you’re not?
What we do now is we leave it up to the providers. What we stress is that if you’re going to use it you can’t use it as a crutch. It’s not your get out of jail free card because you don’t know whether or not it’s going to work and most likely it’s not. Basically, we said we’ll leave it up to you guys but most likely will not prolong the apneic period in the majority of patients. We try and emphasize proper pre-oxygenation because we know that will prolong the apneic period, and if you can’t perform proper pre-ox, then definitely use apo-ox.
So it’s not in your 31 point check list?
No its not, but you can add it if you like.
Last comments?
Really this was a real-world study of apneic oxygenation with the points being, number one, we intubate patients fairly quickly in real life. If you can intubate in 60-90 seconds there’s no need to wait longer than that. If you can intubate a grade 2 view and you’re confident in that, there’s no need to prolong the apneic period to get the grade 1 view. Same thing with a grade 3 to a grade 2. If you’re confident in your adjuncts, then just intubate the patient. The other main point being that proper pre-oxygenation will likely negate the effects of apneic oxygenation. The biggest take-away is that providers need to do proper pre-oxygenation. If they do this, then 9 out of 10 times you will have enough time to intubate regardless of apneic oxygenation.
![]() EmergeNcy Department use of Apenic Oxygenation versus usual care during rapid sequence intubation: a randomized controlled trial. Caputo et al. Annals of EM, Aug 2017
EmergeNcy Department use of Apenic Oxygenation versus usual care during rapid sequence intubation: a randomized controlled trial. Caputo et al. Annals of EM, Aug 2017
![]() RebelEM Article Review by Salim. “The ENDAO Trial: Is Apneic Oxygenation a Futile Intervention in ED RSI?”
RebelEM Article Review by Salim. “The ENDAO Trial: Is Apneic Oxygenation a Futile Intervention in ED RSI?”
Article and Interview by Terren Trott @tsquaredmd
