Comparison of Etomidate and Ketamine for Induction During Rapid Sequence Intubation of Adult Trauma Patients
Upchurch et al. Annals of Emergency Medicine. January 2017.
Objective: to compare outcomes between etomidate and ketamine in trauma patients
Methods: retrospective review of a change in protocol from etomidate to ketamine for induction in trauma patients. From January 2011 to December 2012, etomidate was the on-protocol induction agent, replaced by ketamine in December 2012 until the study end in December 2014. Clinicians were able to choose off-protocol induction agents as deemed necessary at any point.
A total of 968 patients requiring intubation in the ED were enrolled; 54% induced with etomidate and 46% with ketamine. Doses for etomidate were 0.3mg/kg and ketamine 1-2mg/kg.
Outcomes: primary outcome was death in the ED or death during hospitalization. Secondary measures included ICU-free days, ventilator-free days, pressor-free days and hospital acquired sepsis, among others.
| Hospital mortality | No Significant Difference |
| ICU days | No Significant Difference |
| Ventilator-free days | No Significant Difference |
| Hospital acquired sepsis | No Significant Difference |
| Need for steroids | No Significant Difference |
| Time to discharge | No Significant Difference |
| First pass success | No Significant Difference |
| Peri-intubation arrest | No Significant Difference |
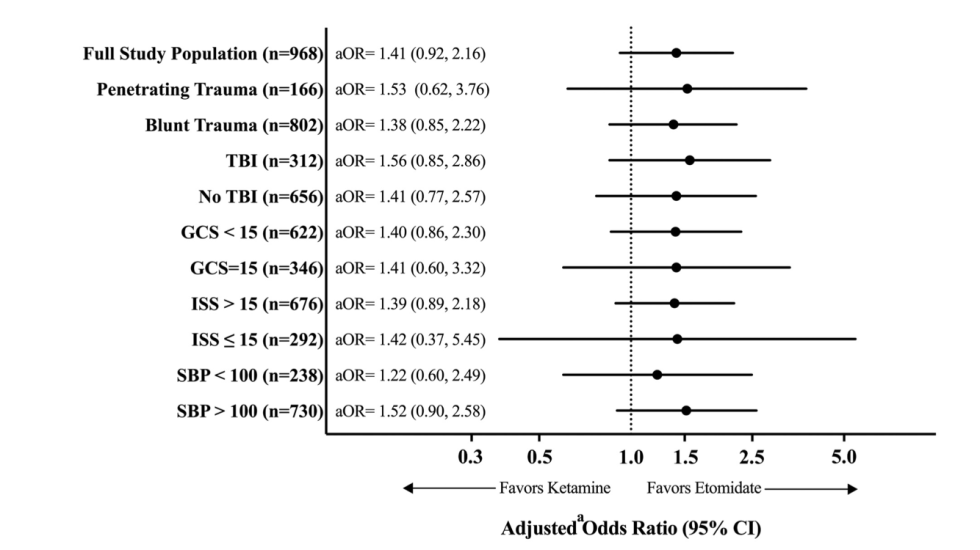
Furthermore, a subgroup pertinent to ketamine folklore was defined as severe head trauma. This group included intracranial hemorrhage, DAI or shear injury on first CT. This group also did not differ from etomidate in mortality, adding to the growing data ketamine is not contraindicated in head trauma.
But! While there was no significant difference, this chart demonstrates the mortality odds ratio in each subgroup with a trend favoring etomidate.
This is, to date, the largest study comparing etomidate and ketamine so it is unlikely that we’ll see a study with higher power than this in the near future.
Discussion:
This is the latest of a few studies showing non-inferiority of etomidate to ketamine or other induction agents. This includes 2009 Lancet article with approx. 220 patients in ‘acutely ill medical patients’ and a Cochrane Review from 2015. Both of these demonstrate similar findings in the primary outcome of mortality as well as minimal differences in secondary outcomes. Etomidate and the discussion of adrenal suppression was not directly addressed in this study other than the need for steroids, which had no difference. Ketamine again was shown to be safe in head trauma despite historical anecdotes. Does this affect my practice? Short answer, yes. It gives me further confidence to broaden my use of ketamine for induction as the body of evidence demonstrating its safety grows in multiple scenarios.
References:
![]() Cameron P. Upchurch. Comparison of Etomidate and Ketamine for Induction during Rapid Sequence Intubation of Adult Trauma Patients. Ann Emerg Med. 2017 Jan; 69(1): 24–33.e2
Cameron P. Upchurch. Comparison of Etomidate and Ketamine for Induction during Rapid Sequence Intubation of Adult Trauma Patients. Ann Emerg Med. 2017 Jan; 69(1): 24–33.e2
![]() Jabre, Patricia et al. Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: a multicentre randomised controlled trial. The Lancet , Volume 374 , Issue 9686 , 293 – 300
Jabre, Patricia et al. Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: a multicentre randomised controlled trial. The Lancet , Volume 374 , Issue 9686 , 293 – 300
![]() Bruder EA, Ball IM, Ridi S, Pickett W, Hohl C. Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients. Cochrane Database of Systematic Reviews 2015, Issue 1.
Bruder EA, Ball IM, Ridi S, Pickett W, Hohl C. Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients. Cochrane Database of Systematic Reviews 2015, Issue 1.
