Association Between Tracheal Intubation During Adult In-Hospital Cardiac Arrest and Survival
Anderson et al. JAMA, January 2017
Objective: to determine whether intubation during adult in-hospital arrest was associated with increased survival to discharge.
Methods: First, there are a lot of details with regards to how this study was performed… and it can get a bit complicated.. The study used data from an AHA sponsored database of cardiac arrest in 668 US based hospitals. From this database, they extracted a total of 108,000 cardiac arrest events from the years 2000 through 2014. Besides demographic information, time to intubation, ROSC, survival to discharge and favorable outcome were recorded. The time to intubation in minutes was also noted.
The data was analyzed in two ways, matched and unmatched. Unmatched data basically looked at raw numbers, such as survival to discharge, between patients who were intubated and those who weren’t, with consideration that 70% of the patients were intubated. Then in the matched analysis, patients that were intubated were matched with near identical demographics to patients who weren’t intubated. This resulted in two groups of 43,000 patients.
Outcomes:
In the unmatched group:
Patients intubated in the first 15 minutes had a lower survival to discharge:
17.0% (intubated) versus 33.2% (not intubated) P<0.01
Patients in the propensity-matched group:
Patients intubated in the first 15 minutes had a lower survival to discharge as well:
19.4% (intubated) versus 16.3% (not intubated) P<0.01
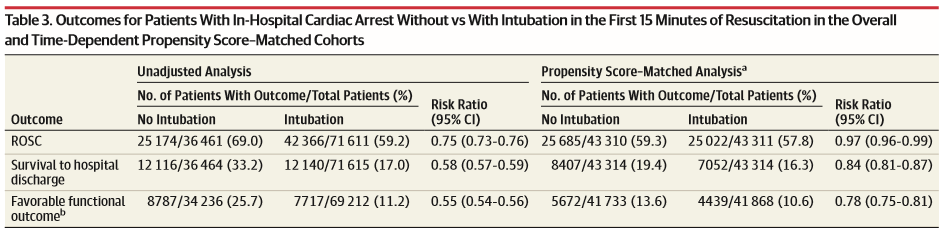
Unmatched and propensity-matched outcomes for intubation vs no intubation with ROSC, survival to discharge and favorable functional outcome.
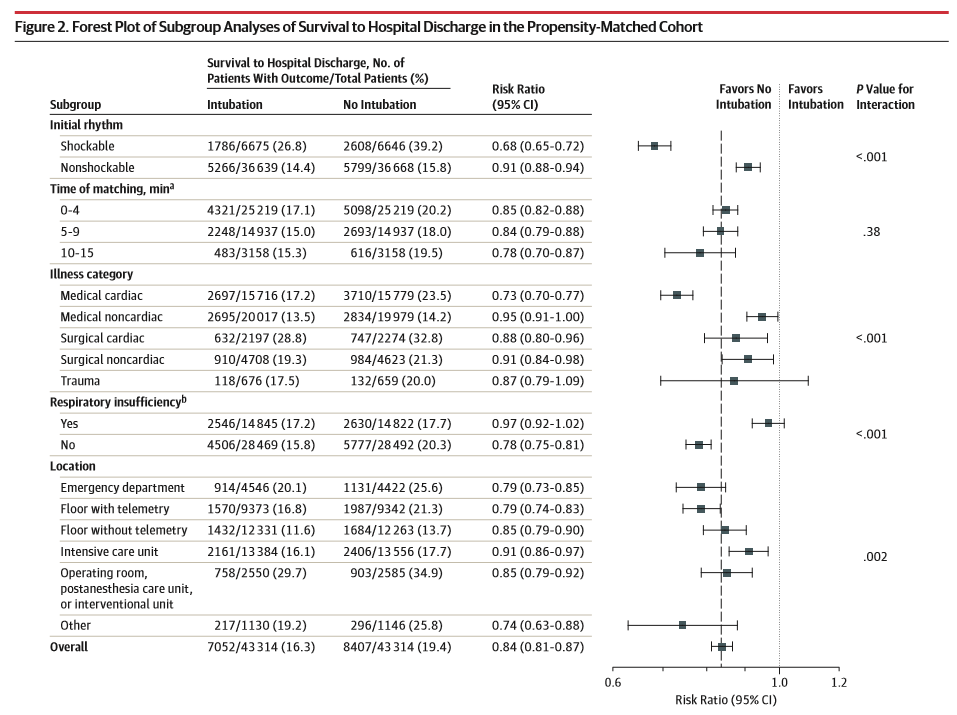
Subgroup analysis in the propensity-matched cohort including shockable vs non-shockable rhythm, time matching, illness category and location.
Discussion:
So obviously the take home point of this article is that there is an association between worse outcomes and intubation during in hospital arrests.. the key word being association. This article actually seems to raise more questions than it answers: is our tried and true mantra of resuscitation – ABC – wrong? Or perhaps what this article suggests is that if the arrest isn’t from an ‘A’ problem, intubation shouldn’t be the priority during resuscitation. The authors provide five key concepts to explain their results:
- Intubation may lead to prolonged interruption in compressions
This is a well-known phenomenon that I’ve seen happen in floor codes repeatedly. At many hospitals, initiatives are put in place to make sure compressions are never interrupted for intubation.
- Intubation may lead to hyperventilation and hyperoxia
Also with merit. Frequently excitement prevails in a room that may lead to bagging too fast. There are several proponents of placing a coding patient on the vent.
- Intubation may delay interventions such as defibrillation and epinephrine.
- Delays to intubation will prevent oxygenation by other means.
In an arrest situation, it can be hard to make the mental acknowledgement that your intubation may be taking too long. Pausing, bagging, or looking for alternative methods of oxygenation may be more important.
- Unrecognized esophageal intubations can lead to fatal outcomes.
Esophageal intubations compose approximately 3% of non-arrest intubations; we can assume that that number is higher in arrests. While methods of confirmation exist with high accuracy in arrests, Murphy’s law seems to prevail…
Of note, the only subgroup that showed a trend supporting intubation was the group with respiratory compromise. Further subgroup analysis showed a strong trend favoring no intubation in patients with shockable rhythms. This highlights focusing on the reversible causes of arrest rather than a potentially lower priority intubation. Also, noted was significantly higher survival in emergency departments compared to all other locations except the OR ;).
In summary, this article provides some very counter intuitive data on intubations in arrest patients. How this will change practice is difficult to say considering how engrained intubation during arrest is.. we’ve all heard, “no one dies without plastic in the mouth,” but clearly this practice is called into question. Would this article alone make you say, let’s just bag the patient until ROSC is obtained? Or perhaps place an LMA? At minimum it reinforces uninterrupted CPR and a focus on reversible causes. Keep in mind that a lot of in-hospital arrests aren’t due to a primary airway problem.
I highly recommend reading this article in its entirety and subscribe to keep updated.
![]() Association Between Tracheal Intubation During Adult In-Hospital Cardiac Arrest and Survival. Anderson et al. JAMA, January 2017
Association Between Tracheal Intubation During Adult In-Hospital Cardiac Arrest and Survival. Anderson et al. JAMA, January 2017
